Lipid subfractions: APO-A1/APO-B: (Pre ASO)!!
Posted: Sat Feb 01, 2025 4:11 am

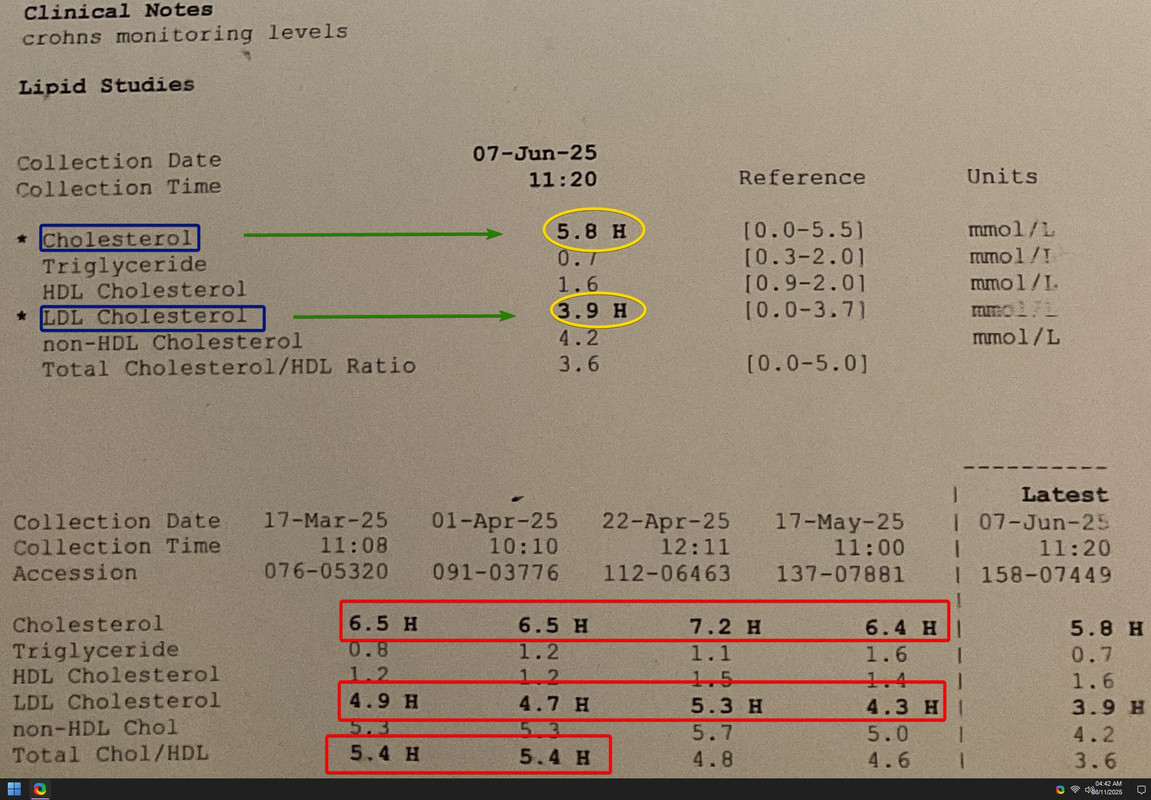
Posting Nik2201's lipids (heterozygous familial hypercholesterolemia), who is undergoing my developed ASO protocol. The test was carried out before ASO, like the earlier ones posted. Would repeat ALL after ASO protocol, APO-A is great and B not that bad either, hoping once repeated after ASO would be as great as was back in '22.

APO-A1 approx. the same, APO-B has doubled...... no issues would hopefully be fixed.
Why am so concerned about normalizing Total Cholesterol etc., since it is the reason/cause for his Crohn's.
Atrial Fibrillation etc. were cured just need to be careful not to disrupt the equilibrium. Like posted before I am treating him like walking on a thin rope, haven't treated all 4/5 conditions in a single person in 37 yrs and that too online.
And haven't witnessed any patient as cooperative as Nik2201 (Btw- I don't consider him as a patient or a member but a great friend), who puts in 200% to my recommendations, with no whining.
Shall request him to repeat all labs after ASO, which shall post.
eDOC!!
PS:
Spent +14 yrs. on a single drug treating humans, could probably have acquired 2 more board certifications.
My personal opinion conv. med is merely palliative, apart from labs.
This and Nik's earlier A-Fib thread is the way to treat and cure a person.
I'm again confused about my specialty since am a conventional neurologist. People are used to specific labels, when I tell them most get confused how a neuro. can treat liver, cardio, endo, renal, autoimmune, ophthalmic, derm, obs/gyn disorders.. list is endless. I probably need to label myself?